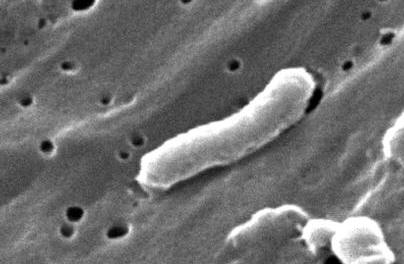
Vibrio choleraeVibrio cholerae is a curve-shaped, Gram-negative bacterium well-known for its ability to cause cholera, a severe bacterial infection in humans (Figure 1). V. cholerae is also motile due to its polar flagellum and makes ATP (an energy molecule) by aerobic respiration if oxygen is present, but is also capable of switching to fermentation - facultative anaerobe. Species belonging to the genus Vibrio are distinguished from Enterobacteria by their flagella, as well as being oxidase positive. They grow in temperatures around 37°C and can survive in conditions as low as 25°C. V. cholerae generally require saltwater to grow properly, but a glucose medium is usually enough for their energy needs.
Figure 1. This scanning electron micrograph depicts a Vibrio cholerae bacterium [22371 X]. V. cholerae live in both marine and freshwater habitats and in association with aquatic animals where they act as parasites to fish, crustaceans (Figure 2), and mammals, including humans. V. cholerae causes diarrhea in humans by a mechanism that involves close adherence to epithelial cells in the small intestines where they secrete an enterotoxin. The enterotoxin, cholera toxin, affects the mucous membranes of the epithelial layer of the intestines, which causes diarrhea. Cholera is a very severe disease that can lead to hypotension, dehydration, and death within a few hours from the first signs of infection, if no treatment is provided. In fact, untreated cholera has a 50% to 60% mortality rate.
Figure 2. Crabs have been a repeated source of cholera in the United States and elsewhere, even though they are rarely eaten raw. The enterotoxin works by activating adenylate cyclase in the epithelial cells. More specifically, it inhibits GTPase enzyme activity so that GDP (an inhibitory molecule) cannot replace the activated G protein which has GTP bound to it in its active state during signal transduction. The activated G protein goes on to activate adenylyl cyclase, producing large amounts of another chemical compound called cAMP. cAMP then activates protein kinase A, an enzyme that induces several different cellular responses, including the release of ions. cAMP also opens plasma membrane calcium channels, so that large amounts of calcium are released into the intestines, leading to an increase in water loss. Cholera toxin modifies the G protein by adding an ADP-ribosyl group to it. This prevents the enzyme GTPase, as mentioned earlier, from hydrolyzing the activated the G protein to a deactivated state which has GDP bound to it, as opposed to GTP. As a result, if the G protein is constantly active, there is persistent activation of adenylyl cyclase and, in turn, a nonregulated rise of intracellular cAMP. O1 or O139 antigen is also a determining factor of V. cholerae virulence, as well as toxin coregulated pilus (TCP), a colonization factor. Both cholera toxin and TCP are controlled by the regulatory protein, ToxR. Another virulence factor that has been described is the mannose-fructose-resistant cell-associated hemagglutinin (MFRHA); however, its action on colonization is not well known (Faruque, 1998). Cholera is especially dangerous to poor areas of the world, such as Bangladesh, where access to doctors or hospitals is limited and sanitation is poor (Figure 3). Cholera has been described as early as the time of Alexander the Great in India. It became more recognized as it spread to other places of the world in the 1800s. Cholera has been found to be endemic in Bengal and is its most likely point of origin. V. cholerae appears to remain in water environments and can be passed to humans, where humans act as a carrier and pass the disease on to others, or back into the water. The spread of V. cholerae has been disputed but it has been suggested that species of the genus Vibrio can change formation and reduce volume in times of stress and starvation, making it hard to detect in water environments. It is estimated that 100000 deaths occur each year due to V. cholerae and many of these deaths are in children. Cholera also targets the immunosuppressed, as well as those who are malnourished; however, it is still dangerous to healthy individuals.
Figure 3. This photograph was taken during a cholera research and nutrition survey in floodwaters of Bangladesh, 1974. Treatment involves feeding the infected person water that includes electrolytes, such as sodium, potassium, calcium ions to make up for the vast amount of electrolytes that are lost as a result of watery diarrhea. Homemade electrolytes can be used, such as table sugar, baking soda, or salt. Tetracycline is the major antibiotic used to treat infection for cholera. Stool samples can be used to test for the presence of V. cholerae in an individual, although treatment will often be administered before laboratory diagnosis due to the virulence of cholera and its rate of spread during major cholera outbreaks (Figure 4). These stools are inoffensive, with a faint fishy odor. They are isotonic with plasma, and contain high levels of sodium, potassium and bicarbonate. They also contain extraordinary quantities of Vibrio cholerae bacterial organisms.
Figure 4. Here, a cup of typical "rice-water" stool from a cholera patient shows flecks of mucus that have settled to the bottom. References: Faruque, S. M., Albert, M. J., & Mekalanos, J. J. (1998). Epidemiology, Genetics, and Ecology of Toxigenic Vibrio cholerae. Microbiology and Molecular Biology Reviews, 62:1301-1314. Bergey, D. H., & Holt, J.G. Bergey's Manual of Determinative Bacteriology. Baltimore: Williams & Wilkins, 1994. |